When used appropriately, blood flow restriction (BFR) training is a safe, feasible, and effective tool, that can enhance muscle function (1,2). For a more detailed discussion on the specific benefits and risks of BFR training, please refer to part 1 of this Blood Flow Restriction Training article. In part 2, we will explore some of the practical recommendations for using BFR resistance training safely and effectively and this will be addressed in the following 5 short sections:
1. Appropriate cuff factors (pressure, type, and width)
2. Exercise intensity, execution and type
3. Exercise frequency, volume, and duration
4. Exercise order and recovery
5. Practical recommendations summary
Appropriate Cuff Factors (Pressure, Type, and Width)
Blood flow is typically restricted to an upper body limb (cuff compression just below the shoulder) or lower body limb (cuff compression at the top of the thigh). Ideally, individuals should use a pneumatic BFR cuff that mechanically controls (with air or gas) and displays (on a dial) the amount of pressure (in mmHg) applied. The goldilocks zone for BFR pressure during resistance training is typically somewhere between 40-80% of arterial occlusion pressure [the pressure where blood flow completely ceases (AOP)]. Whilst cuff material (elastic vs nylon) does not impact required pressure (1), cuff width (5-18cm) does.
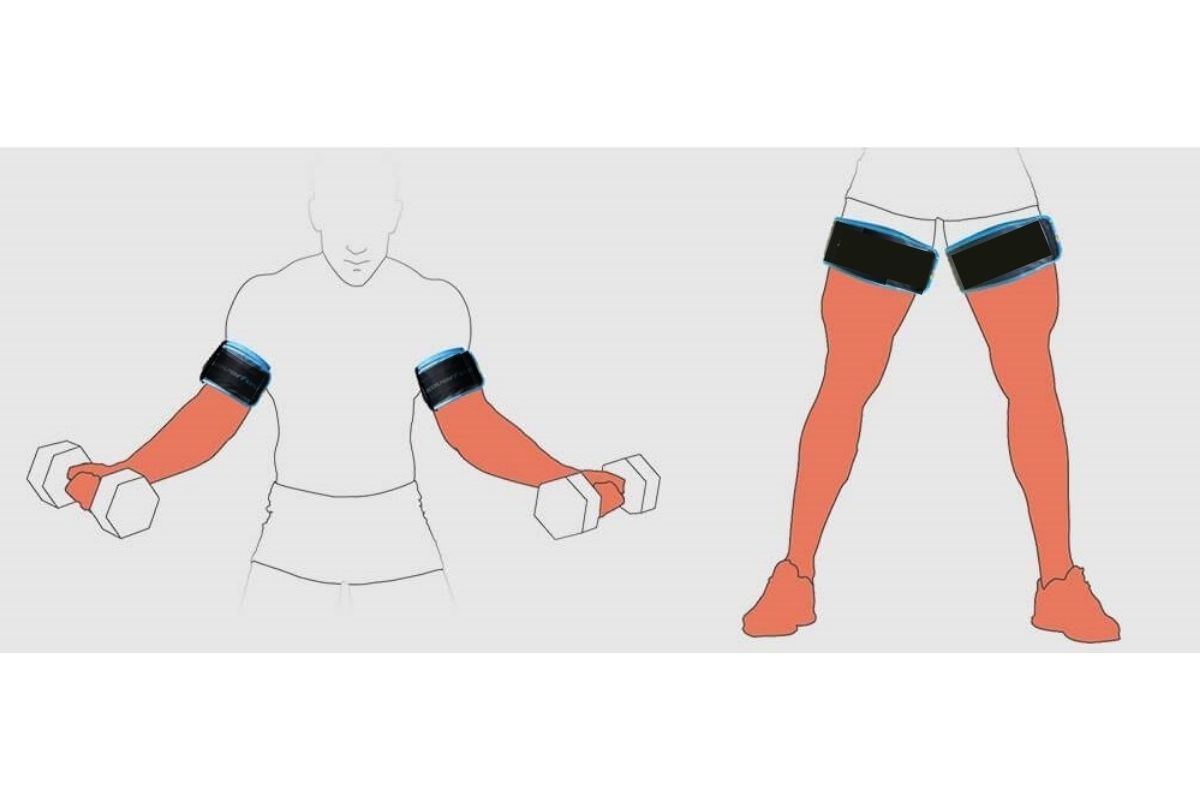
Image from RecoverFun
Wider cuffs require less pressure (closer to 40% AOP) to reduce blood flow because more vasculature is being compressed at a given pressure. Furthermore, wider cuffs may also lead to less skin pinching, nerve compression, and numbness as pressure is distributed across a greater surface area (3). Therefore, it is worth re-stating that narrower cuffs should be applied with less pressure to avoid unnecessary damage to both neural and vascular tissue. Despite their benefits over narrower cuffs, wider cuffs may inhibit movement during exercise. Finally, a larger limb (e.g. leg vs arm, larger vs smaller individual), and a proximally located muscle in relation to the cuff (e.g. the glutes when the cuff is inflated around the thigh), may require a greater amount of pressure (closer to 80% AOP) to reduce muscle blood flow.
Exercise Intensity, Execution, and Type
The ideal intensity for BFR resistance training is typically prescribed between 20-40% of one-repetition maximum (1-RM) (1), although intensity may differ depending on targeted muscle group and applied pressure. In any case, BFR resistance training is not advised at ≥40% 1-RM because high intensity resistance training produces huge increases in blood pressure (arterial pressure can rise to ~320/250 mmHg during bilateral leg press at ≥80% 1-RM) (4).
Alternatively, individuals could simply select a resistance exercise intensity/ cuff pressure, where they can gradually work up to concentric failure (cannot produce another repetition) for a particular movement. Typically, this involves repetition speeds of 1 second concentric, and 2 seconds eccentric. For this reason, BFR is more suited to simpler movements that are easier to perform (e.g. single joint isolation exercises), especially towards the end of a set when muscle swelling can make force production difficult.
Individuals can select a variety of exercise modalities during BFR training like dumbbells, resistance machines, and resistance bands. When using resistance bands however, individuals should be mindful of additional skin compression from the band (especially around the hands and feet).
Exercise Frequency, Volume, and Duration
The intense BFR approach involves using BFR training 1-2 times per day for 1-3 weeks (1). In contrast, the moderate BFR approach involves using BFR training 2-3 times per week for 3 weeks or longer (1). Whilst there is no safety limit regarding how many exercises BFR can be used during a session, individuals should be mindful that there are only 2 primary sites where a BFR cuff can be tightened (at the top of the thigh and just below the shoulder). This limited number of sites means the same spot will likely be compressed for different exercises (leg curl and leg extension both require restriction at the top of the thigh). Individuals using BFR training as their primary training modality (multiple BFR exercises at the same compression site) should be extra vigilant for numbness and thrombosis (pale skin) (2). For a given exercise, a muscle should ideally be under restriction for 5-10 minutes to achieve the discussed benefits. This typically involves 60-75 repetitions spread out over 2-4 sets of 15-30 reps. An ideal rep scheme is 30, 15, 15, 15, but as previously stated, individuals should work to concentric failure (cannot produce another repetition) for a particular movement.

Exercise Order and Recovery
A general range of 30-60s rest is recommended between sets when using BFR resistance training (1). During such rest time, it is the individual’s choice whether to keep the cuff inflated or deflated. Importantly, this does not impact the benefits, but may reduce the experience of adverse symptoms (1). In any case, a limb should be under compression for no longer than 10 minutes. After such time the cuff should be immediately deflated, allowing blood flow to return to the muscle in-between exercises. It is still advisable to take rest days between sessions to allow the acute recovery of muscle and neural tissues. General activity (e.g. light walking) is encouraged on rest days to promote blood flow to muscles on non-training days. Furthermore, strategically planned periods without BFR are also advisable. Initially, individuals could adopt a 1:1 approach, i.e. 3 weeks of BFR training, followed by 3 weeks without BFR.
Practical Recommendations Summary
The practical recommendations for using BFR in practice are as follows (1):
Cuff Factors: Using a pneumatic cuff, blood flow to a limb should be restricted (e.g. at the top of the thigh or just below the shoulder) for ≤10 minutes with a pressure of 40-80% arterial occlusion pressure (AOP). The required pressure may vary depending on cuff width, limb size, exercise intensity, and the location of the target muscle in relation to the cuff (e.g. proximal).
Intensity: Work at 20-40% of 1-RM, or an intensity that allows an individual to build up to concentric failure. Intensity may differ depending on cuff pressure, muscle group, and desired training goal (strength or hypertrophy).
Execution: Use repetition speeds of 1 second concentric, and 2 seconds eccentric.
Type: Perform simple, single joint isolation exercises (e.g. leg extension) using a variety of modalities (e.g. dumbbells, resistance machines, and resistance bands).
Frequency: Use either an intense (1-2 times/ day for 1-3 weeks), or moderate approach (2-3 times/ week for ≥3 weeks).
Volume: Perform 60-75 repetitions (2-4 sets of 15-30 reps), or until concentric failure.
Recovery: Use an inter-set rest period of 30-60s. Cuff deflation during rest is not required, but should be used to one’s experience of symptoms (numbness and thrombosis). Rest days (performing light activity), and periods without BFR (1:1 ratio) should also be used to alleviate adverse symptoms.
Order: Care should be taken not to perform too many consecutive exercises or sessions using the same muscle group or compression site.
Despite the benefits of appropriate BFR training, some individuals may find the experience too uncomfortable. As such, this training modality should not be viewed as an all-conquering solution to gain muscle size and strength. Instead, BFR training should be viewed as another tool in training box that can be used with some individuals, in some scenarios and for some specific goals. Some of the appropriate scenarios may include:
• individuals that are recovering from an injury, illness, or surgery
• individuals that struggle to perform high intensity resistance exercise
• individuals for whom high intensity resistance exercise is contra-indicated (e.g. those suffering from inflammatory disease)
• individuals for whom the loss of muscle mass is accelerated (e.g. frail older adults with no cardiovascular contraindications)
• highly trained individuals whose progress is beginning to stall or plateaux
It is important to underline the fact that even though clinically vulnerable populations will likely obtain the greatest benefit from BFR resistance training, they will also be at the greatest risk of experiencing the adverse effects (e.g. numbness and thrombosis). This should be taken into account by those wishing to use BFR resistance training.
Disclaimer: This article is not intended as an endorsement of blood flow restriction training. Instead this article is an evidence-based discussion about the benefits and risks of this novel training tool. If an individual is considering using blood flow restriction training as part of their training program, this should be done with the approval of the individuals healthcare provider, and under the supervision of a suitably qualified and experienced health and fitness professional.
References
1. Patterson, S.D., Hughes, L., Warmington, S., Burr, J., Scott, B.R., Owens, J., Abe, T., Nielsen, J.L., Libardi, C.A., Laurentino, G. and Neto, G.R., 2019. Blood flow restriction exercise: considerations of methodology, application, and safety. Frontiers in physiology, 10, p.533.
2. Sato, Y., 2005. The history and future of KAATSU training. International Journal of KAATSU Training Research, 1(1), pp.1-5.
3. Rabe, E., Partsch, H., Morrison, N., Meissner, M.H., Mosti, G., Lattimer, C.R., Carpentier, P.H., Gaillard, S., Jünger, M., Urbanek, T. and Hafner, J., 2020. Risks and contraindications of medical compression treatment–A critical reappraisal. An international consensus statement. Phlebology, 35(7), pp.447-460.
4. MacDougall, J.D., Tuxen, D.S.D.G., Sale, D.G., Moroz, J.R. and Sutton, J.R., 1985. Arterial blood pressure response to heavy resistance exercise. Journal of applied Physiology, 58(3), pp.785-790.
